
Page 255 - Cardiac Nursing
P. 255
009
009
6/2
0/0
6/2
0:4
7 A
0:4
1
1
q
q
q
44.
44.
3
0/0
3
xd
xd
7 A
p
p
A
31
A
ara
ara
t
p
t
Pa
g
Pa
M
M
e 2
31
e 2
g
g
LWBK340-c10_
LWB
LWB K34 0-c 10_ pp211-244.qxd 30/06/2009 10:47 AM Page 231 Aptara
10_
0-c
K34
p
21
1-2
1-2
21
p
C HAPTER 1 0 / History Taking and Physical Examination 231
than does percussion. Percussion is most useful in the rare in- centimeters from the sternum or the MCL. Determine whether it
6
stance where dextrocardia is suspected. The room should be quiet occurs in systole or diastole by timing it with the carotid pulse or
and permit privacy. Both the patient and the examiner should be the heart sounds. In general, retractions are more easily seen, and
in comfortable positions before beginning the examination. pulsations are more easily palpated.
When visible, the normal apex impulse can be seen within the
Topographic Anatomy fifth ICS at or just medial to the MCL. It is an early systolic pul-
sation with a rapid upstroke and downstroke. A late systolic re-
Knowledge of the topographic anatomy of the cardiac and vas- traction, 1 to 2 cm long, in the fourth or fifth ICS may also be
cular structures is essential to understanding the clinical find- normally seen and is produced by ventricular emptying. The apex
ings. The left ventricle is primarily a posterior structure and is impulse cannot be seen in every patient. It is easily detected in
evaluated on the anterior chest wall at the cardiac apex, which is thin patients, whereas it may not be visible in those who are obese
normally in the fifth intercostal space (ICS) at, or slightly me- or have large breasts or barrel chests. An apex impulse that is be-
dial to, the mid-clavicular line (MCL). The right ventricle is an- low the fifth ICS, lateral to the MCL, or seen in more than one
terior to the left ventricle and underlies the sternum and the ICS represents left ventricular enlargement.
lower left sternal border at the fourth and fifth ICS. The right Slight movement over the sternum or the epigastrium can be
atrium is just lateral to the lower right sternal border. The out- normal in thin people and in those with fever or anemia who may
flow tracts of both ventricles underlie the third left ICS (Erb’s have hyperdynamic heartbeats. A sternal rise that is sustained after
point). The main pulmonary artery underlies the second left ICS, systole begins usually indicates right ventricular enlargement. Pul-
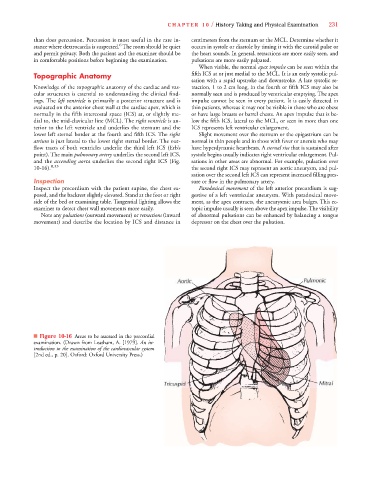
and the ascending aorta underlies the second right ICS (Fig. sations in other areas are abnormal. For example, pulsation over
10-16). 8,33 the second right ICS may represent an aortic aneurysm, and pul-
sation over the second left ICS can represent increased filling pres-
Inspection sure or flow in the pulmonary artery.
Inspect the precordium with the patient supine, the chest ex- Paradoxical movement of the left anterior precordium is sug-
posed, and the backrest slightly elevated. Stand at the foot or right gestive of a left ventricular aneurysm. With paradoxical move-
side of the bed or examining table. Tangential lighting allows the ment, as the apex contracts, the aneurysmic area bulges. This ec-
examiner to detect chest wall movements more easily. topic impulse usually is seen above the apex impulse. The visibility
Note any pulsations (outward movement) or retractions (inward of abnormal pulsations can be enhanced by balancing a tongue
movement) and describe the location by ICS and distance in depressor on the chest over the pulsation.
■ Figure 10-16 Areas to be assessed in the precordial
examination. (Drawn from Leatham, A. [1979]. An in-
troduction to the examination of the cardiovascular system
[2nd ed., p. 20]. Oxford: Oxford University Press.)