
Page 342 - Cardiac Nursing
P. 342
Pa
g
M
Pa
e 3
e 3
g
g
M
1
1
/09
/09
0 P
0 P
0:3
0:3
a
a
ara
ara
c.
c.
In
In
t
A
A
18
18
p
t
p
p
0-3
LWB
LWBK340-c15_
32.
LWB K34 0-c 15_ pp300-332.qxd 6/29/09 10:30 PM Page 318 Aptara Inc.
0-3
K34
p
30
30
0-c
15_
p
32.
6
xd
6
/29
/29
xd
q
q
q
318 P A R T III / Assessment of Heart Disease
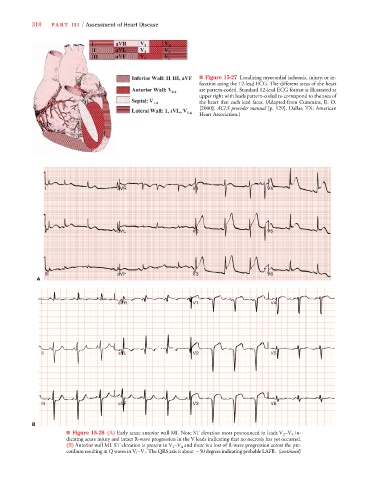
■ Figure 15-27 Localizing myocardial ischemia, injury, or in-
farction using the 12-lead ECG. The different areas of the heart
are pattern-coded. Standard 12-lead ECG format is illustrated at
upper right with leads pattern-coded to correspond to the area of
the heart that each lead faces. (Adapted from Cummins, R. O.
[2000]. ACLS provider manual [p. 129]. Dallas, TX: American
Heart Association.)
VR
VRR
VR
V
V
V
V
V
VR
V
V
V
V V V V V V V V V V V V V V V V V V V1
R
V V V V V V V V V V
VR
V
V
V
aV
R
a a a a a a a a a a a a a a a a a a a a a
aV
R
R
R
R
aV
R
R
R
R
I I I I I I I I I I aV R V V V V V V V V V V V V V 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 V4 4 4 4 4 4 4 4 4 4 4 4 4 4
R
R
R
R R R R R R R R R R
V V V V V V V V V V V V V V V V V V V V V V V V V V V V V V V V
V
V4
V V4
V
V
V
V
V4
R
L L L L
L
L
L
L
L
L
V
V
V
V
V
V
VL
I I I I I I I I I I I I I I I II I aV L V V V V V V V V V V V V V V V V V V V V2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 V5 5 5 5 5 5 5 5 5 5 5 5 5
VLL
VL
VL
V5
aV
V5
a a a a a a a a a a a a a a a a
V V V V V V V V V V V V V V V V V V V V V V V V V V
aV
V
V
V
aV
V5
V
V
V
V V V V V V V V
F
F
F
F
F
VF
F
F F F F
F
F
F
aV
aV
a a a a a a a a a a a a a a
V
aV
V6
VF
F
V
V6
V
VFF
V
V
V
V
V
V V V V V V V V V V V V V V V V3
V
V V V V V V V V
V
V V V V V V V V V V V V V V V V V V V V V V V V V V V V
V6
VF
V
V
I I I I II II II II I I I I I I I I I I I I I I I I aV F V V V V V V V 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 V6 6 6 6 6 6 6 6 6 6 6 6 6
A
V44
V V V V4
V V V V4
V4
V4
V V V V4
V V V1
V V V1
R
V V V1
V1
V V V1
V1
R
R
R
R
R
R
R
V
VR
V
V
V
V
V
V
V
V
V
V
a a aVR
aVRVR
aVR
I I I I I I I I I I I a a aVR V11 1 1 1 V V V V4 4 4 4 4 4 4 4
a a aV
V
V
V
V
VR
V
a a aV
a a aV
V V V V5
aVV
V
VL
VL
VL
V V V V5
V22
V V V2
II II II II II II II II II a a aV L V V V2 2 2 2 2 2 V55 5 5 5 5 5
V V V2
V V5
V V V V5
V V2
aV
V
V
V
L
L
V
VL
VL
V
V
V
VL
V
V
V
V
V
V
VF
V
a a aV
aVVVF
V
V6
V V V V6
V V V V6
V66
III I I III II III II III III III II I a a aV F F F F F F F F F F F F V V V3 3 3 3 3 3 V6 6 6 6 6 6
V
V V V V6
V
V
V3
V
V
V
V
V
V
V3
V
V
VF
V
aV
aV
V V V3
V V V3
V33
V
V
B
V
■ Figure 15-28 (A) Early acute anterior wall MI. Note ST elevation most pronounced in leads V 2 –V 5 in-
dicating acute injury and intact R-wave progression in the V leads indicating that no necrosis has yet occurred.
V
(B) Anterior wall MI. ST elevation is present in V 1 –V 4 and there is a loss of R-wave progression across the pre-
cordium resulting in Q waves in V 1 –V 3 . The QRS axis is about 50 degrees indicating probable LAFB. (continued)
V