
Page 345 - Cardiac Nursing
P. 345
0 P
0 P
0:3
1
0:3
Pa
g
Pa
M
M
6
6
xd
q
xd
/09
1
/09
/29
/29
g
ara
a
ara
t
t
c.
c.
In
a
In
21
21
e 3
g
e 3
p
p
p
A
A
q
30
0-3
0-3
30
LWB K34 0-c 15_ pp300-332.qxd 6/29/09 10:30 PM Page 321 Aptara Inc.
p
p
LWB
32.
32.
q
15_
LWBK340-c15_
K34
0-c
C HAPTER 1 5 / Electrocardiography 321
V44
V4
V4 4 4 4 4
V V V V V V V V V V V V
I I I I I I I aV R V V V V V V V1 1 1 1 1 1 1
a a a a a a a a
V
V
aV
V
aV
V V V VR
R R R R R R R R R R R R
V
V
I I I I I I I I I I I I II a a a a a a a a aV L V V V V V V V V V2 2 2 2 2 2 2 2 2 2 V5 5 5 5 5 5
V
V
V V V VL
aV
L L L L L L L L
aV
V
V5
V V V V V V V V V V V V V V V
V55
V5
I I I I I I I I I I I I III aV F V 3 3 3 3 3 3 3 V6 6 6 6 6
V V V V V V V V V V V V
V66
V V V V V V V3
aV
a a a a a a a a
F F F F F F F F F
V6
aV
V V VF
V
V
A
I I I I a a a a a a a a aV R R R R R R R R R R R R
R
R
VR
VR
a a
VR
V
VRR
V V V V V
V V4
V V V V V V V V V V V V V
V4
V1
V V V V V V V V V V V
V4
V1
4 4 4
4
V1 1 1 1 1 V 4
V11
V
VL
5 5 5 5
V
V V V V V
5
5
a a
a a a a a a a a aV L L L L L L L L L V V V V V V V V V V 2 2 2 2 2 V5
VLL
V
V
V5
V5
VL
VL
V5
V V V V V V V V V V V V V
V22
V2
V2
V2
I I I I I I I I
6
6
V6
V
V V V V V V V V V V V V V
V
6 6 6 6
V6
V3
V3
V V V V V V V V V V V 3 3 3 3 3 3 3 3 3 V6
V3
V33
V6
a a a a a a a a a a aV F F F F F F F F F
V V V V V
VF
VFF
V
VF
VF
B I I I I I I I I I I I I
4R
R
4RR
V4
V V V V V V V V V V V4
4
4
V4
V4
V V4 R R R R R R R R R
4R
V V4
V5
V V V V V V V V V V V V V5
R
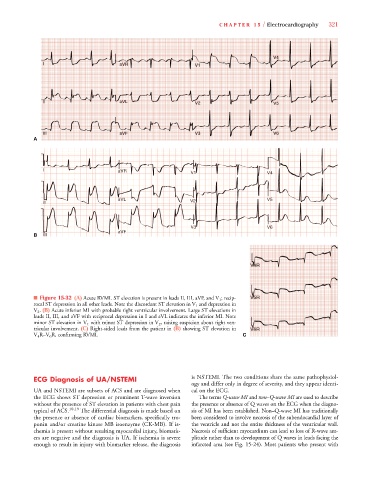
■ Figure 15-32 (A) Acute RVMI. ST elevation is present in leads II, III, aVF, and V 1 ; recip- V5 R R R R R R R R
5
5R
5R
5RR
5R
5
V V V V
V V5
5
5
rocal ST depression in all other leads. Note the discordant ST elevation in V 1 and depression in
V
V 2 . (B) Acute inferior MI with probable right ventricular involvement. Large ST elevations in
leads II, III, and aVF with reciprocal depression in I and aVL indicates the inferior MI. Note
V
minor ST elevation in V 1 with minor ST depression in V 2 , raising suspicion about right ven-
tricular involvement. (C) Right-sided leads from the patient in (B) showing ST elevation in V6 R R R R R R R R
V6
6
V6
V V V V V V V V V V V V V V V
V6
6RR
6R
6R
R
6R
6
V 4 R–V 6 R, confirming RVMI.
V C
ECG Diagnosis of UA/NSTEMI is NSTEMI. The two conditions share the same pathophysiol-
ogy and differ only in degree of severity, and they appear identi-
UA and NSTEMI are subsets of ACS and are diagnosed when cal on the ECG.
the ECG shows ST depression or prominent T-wave inversion The terms Q-wave MI and non–Q-wave MI are used to describe
without the presence of ST elevation in patients with chest pain the presence or absence of Q waves on the ECG when the diagno-
typical of ACS. 10,19 The differential diagnosis is made based on sis of MI has been established. Non–Q-wave MI has traditionally
the presence or absence of cardiac biomarkers, specifically tro- been considered to involve necrosis of the subendocardial layer of
ponin and/or creatine kinase MB isoenzyme (CK-MB). If is- the ventricle and not the entire thickness of the ventricular wall.
chemia is present without resulting myocardial injury, biomark- Necrosis of sufficient myocardium can lead to loss of R-wave am-
ers are negative and the diagnosis is UA. If ischemia is severe plitude rather than to development of Q waves in leads facing the
enough to result in injury with biomarker release, the diagnosis infarcted area (see Fig. 15-24). Most patients who present with