
Page 388 - Cardiac Nursing
P. 388
2:1
6 A
2:1
1
1
6 A
Pa
Pa
Pa
M
M
1
xd
6
xd
q
q
6
/09
/09
/09
/30
/30
ara
ara
t
p
t
a
c.
c.
In
a
In
p
e 3
e 3
g
g
g
64
A
p
A
64
64
LWB K34 0-c 16_ p p pp333-387.qxd 6/30/09 12:16 AM Page 364 Aptara Inc.
LWB
33
33
0-c
16_
LWBK340-c16_
K34
87.
3-3
3-3
q
87.
364 P A R T III / Assessment of Heart Disease
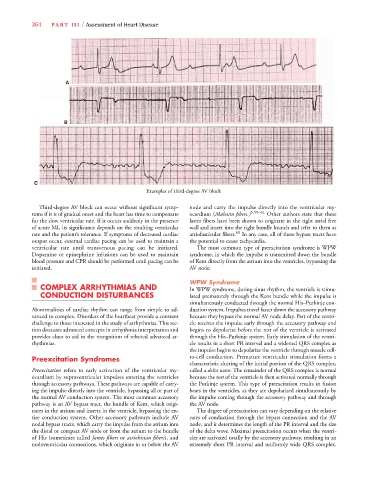
A
B
C
Examples of third-degree AV block
Third-degree AV block can occur without significant symp- node and carry the impulse directly into the ventricular my-
toms if it is of gradual onset and the heart has time to compensate ocardium (Mahaim fibers.) 5,59–61 Other authors state that these
for the slow ventricular rate. If it occurs suddenly in the presence latter fibers have been shown to originate in the right atrial free
of acute MI, its significance depends on the resulting ventricular wall and insert into the right bundle branch and refer to them as
rate and the patient’s tolerance. If symptoms of decreased cardiac atriofascicular fibers. 60 In any case, all of these bypass tracts have
output occur, external cardiac pacing can be used to maintain a the potential to cause tachycardia.
ventricular rate until transvenous pacing can be initiated. The most common type of preexcitation syndrome is WPW
Dopamine or epinephrine infusions can be used to maintain syndrome, in which the impulse is transmitted down the bundle
blood pressure and CPR should be performed until pacing can be of Kent directly from the atrium into the ventricles, bypassing the
initiated. AV node.
WPW Syndrome
COMPLEX ARRHYTHMIAS AND In WPW syndrome, during sinus rhythm, the ventricle is stimu-
CONDUCTION DISTURBANCES lated prematurely through the Kent bundle while the impulse is
simultaneously conducted through the normal His–Purkinje con-
Abnormalities of cardiac rhythm can range from simple to ad- duction system. Impulses travel faster down the accessory pathway
vanced to complex. Disorders of the heartbeat provide a constant because they bypass the normal AV node delay. Part of the ventri-
challenge to those interested in the study of arrhythmias. This sec- cle receives the impulse early through the accessory pathway and
tion discusses advanced concepts in arrhythmia interpretation and begins to depolarize before the rest of the ventricle is activated
provides clues to aid in the recognition of selected advanced ar- through the His–Purkinje system. Early stimulation of the ventri-
rhythmias. cle results in a short PR interval and a widened QRS complex as
the impulse begins to depolarize the ventricle through muscle cell-
Preexcitation Syndromes to-cell conduction. Premature ventricular stimulation forms a
characteristic slurring of the initial portion of the QRS complex,
Preexcitation refers to early activation of the ventricular my- called a delta wave. The remainder of the QRS complex is normal
ocardium by supraventricular impulses entering the ventricles because the rest of the ventricle is then activated normally through
through accessory pathways. These pathways are capable of carry- the Purkinje system. This type of preexcitation results in fusion
ing the impulse directly into the ventricle, bypassing all or part of beats in the ventricles, as they are depolarized simultaneously by
the normal AV conduction system. The most common accessory the impulse coming through the accessory pathway and through
pathway is an AV bypass tract, the bundle of Kent, which origi- the AV node.
nates in the atrium and inserts in the ventricle, bypassing the en- The degree of preexcitation can vary depending on the relative
tire conduction system. Other accessory pathways include AV rates of conduction through the bypass connection and the AV
nodal bypass tracts, which carry the impulse from the atrium into node, and it determines the length of the PR interval and the size
the distal or compact AV node or from the atrium to the bundle of the delta wave. Maximal preexcitation occurs when the ventri-
of His (sometimes called James fibers or atriohisian fibers), and cles are activated totally by the accessory pathway, resulting in an
nodoventricular connections, which originate in or below the AV extremely short PR interval and uniformly wide QRS complex.