
Page 389 - Cardiac Nursing
P. 389
87.
3-3
3-3
87.
q
q
q
M
p
Pa
Pa
p
M
33
33
xd
1
1
/09
1
6 A
2:1
2:1
/09
6
6 A
xd
6
/09
/30
/30
Pa
LWBK340-c16_
K34
0-c
LWB
ara
ara
LWB K34 0-c 16_ pp333-387.qxd 6/30/09 12:16 AM Page 365 Aptara Inc.
c.
c.
16_
In
a
a
In
t
65
e 3
65
65
g
g
e 3
g
p
t
p
A
A
p
C HAPTER 1 6 / Arrhythmias and Conduction Disturbances 365
A A B B
(
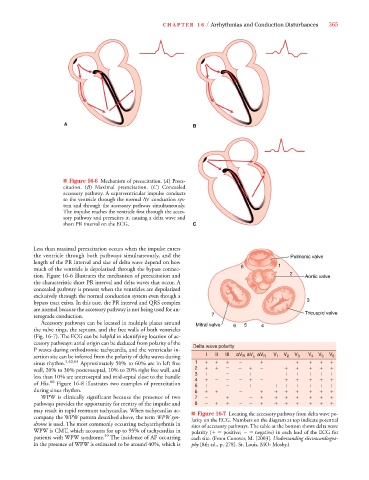
■ Figure 16-6 Mechanism of preexcitation. (A( ) Preex-
citation. (B) Maximal preexcitation. (C ) Concealed
accessory pathway. A supraventricular impulse conducts
to the ventricle through the normal AV conduction sys-
tem and through the accessory pathway simultaneously.
The impulse reaches the ventricle first through the acces-
sory pathway and preexcites it, causing a delta wave and
short PR interval on the ECG. C
Less than maximal preexcitation occurs when the impulse enters
the ventricle through both pathways simultaneously, and the Pulmonic valve
length of the PR interval and size of delta wave depend on how 1
much of the ventricle is depolarized through the bypass connec- 8
tion. Figure 16-6 illustrates the mechanism of preexcitation and 2 Aortic valve
the characteristic short PR interval and delta waves that occur. A
concealed pathway is present when the ventricles are depolarized
exclusively through the normal conduction system even though a
bypass tract exists. In this case, the PR interval and QRS complex 3
are normal because the accessory pathway is not being used for an- Tricuspid valve
terograde conduction. 7
Accessory pathways can be located in multiple places around Mitral valve 6 5 4
the valve rings, the septum, and the free walls of both ventricles
(Fig. 16-7). The ECG can be helpful in identifying location of ac-
cessory pathways: atrial origin can be deduced from polarity of the Delta wave polarity
P waves during orthodromic tachycardia, and the ventricular in-
L
R
sertion site can be inferred from the polarity of delta waves during I II III aV aV aV R V 1 V 2 V 3 V 4 V 5 V 6
sinus rhythm. 5,62,63 Approximately 50% to 60% are in left free 1
wall, 20% to 30% posteroseptal, 10% to 20% right free wall, and 2
less than 10% are anteroseptal and mid-septal close to the bundle 3
4
of His. 60 Figure 16-8 illustrates two examples of preexcitation 5
during sinus rhythm. 6
WPW is clinically significant because the presence of two 7
pathways provides the opportunity for reentry of the impulse and 8
may result in rapid reentrant tachycardias. When tachycardias ac- ■ Figure 16-7 Locating the accessory pathway from delta wave po-
company the WPW pattern described above, the term WPW syn- larity on the ECG. Numbers on the diagram at top indicate potential
drome is used. The most commonly occurring tachyarrhythmia in sites of accessory pathways. The table at the bottom shows delta wave
WPW is CMT, which accounts for up to 95% of tachycardias in polarity (
positive; negative) in each lead of the ECG for
patients with WPW syndrome. 59 The incidence of AF occurring each site. (From Conover, M. [2003]. Understanding electrocardiogra-
in the presence of WPW is estimated to be around 40%, which is phy [8th ed., p. 278]. St. Louis, MO: Mosby.)