
Page 386 - Cardiac Nursing
P. 386
6 A
M
6 A
2:1
2:1
Pa
g
Pa
M
Pa
1
/30
/30
6
xd
6
1
1
/09
/09
/09
g
ara
a
ara
t
t
c.
c.
In
a
In
p
62
62
e 3
g
e 3
p
p
A
62
A
xd
33
LWB
3-3
33
K34
LWBK340-c16_
16_
0-c
q
87.
LWB K34 0-c 16_ p p pp333-387.qxd 6/30/09 12:16 AM Page 362 Aptara Inc.
q
87.
q
3-3
362 P A R T III / Assessment of Heart Disease
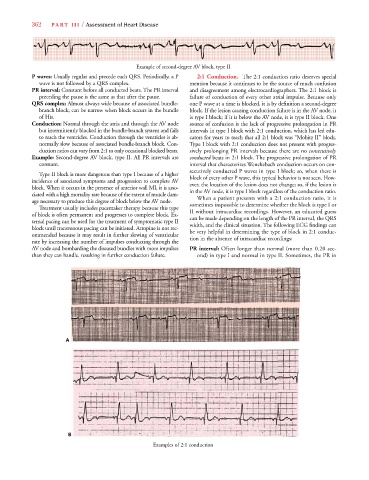
Example of second-degree AV block, type II
P waves: Usually regular and precede each QRS. Periodically, a P 2:1 Conduction. The 2:1 conduction ratio deserves special
wave is not followed by a QRS complex. mention because it continues to be the source of much confusion
PR interval: Constant before all conducted beats. The PR interval and disagreement among electrocardiographers. The 2:1 block is
preceding the pause is the same as that after the pause. failure of conduction of every other atrial impulse. Because only
QRS complex: Almost always wide because of associated bundle- one P wave at a time is blocked, it is by definition a second-degree
branch block; can be narrow when block occurs in the bundle block. If the lesion causing conduction failure is in the AV node, it
of His. is type I block; if it is below the AV node, it is type II block. One
Conduction: Normal through the atria and through the AV node source of confusion is the lack of progressive prolongation in PR
but intermittently blocked in the bundle-branch system and fails intervals in type I block with 2:1 conduction, which has led edu-
to reach the ventricles. Conduction through the ventricles is ab- cators for years to teach that all 2:1 block was “Mobitz II” block.
normally slow because of associated bundle-branch block. Con- Type I block with 2:1 conduction does not present with progres-
duction ratios can vary from 2:1 to only occasional blocked beats. sively prolonging PR intervals because there are no consecutively
Example: Second-degree AV block, type II. All PR intervals are conducted beats in 2:1 block. The progressive prolongation of PR
constant. interval that characterizes Wenckebach conduction occurs on con-
secutively conducted P waves in type I block; so, when there is
Type II block is more dangerous than type I because of a higher
incidence of associated symptoms and progression to complete AV block of every other P wave, this typical behavior is not seen. How-
block. When it occurs in the presence of anterior wall MI, it is asso- ever, the location of the lesion does not change; so, if the lesion is
ciated with a high mortality rate because of the extent of muscle dam- in the AV node, it is type I block regardless of the conduction ratio.
age necessary to produce this degree of block below the AV node. When a patient presents with a 2:1 conduction ratio, it is
Treatment usually includes pacemaker therapy because this type sometimes impossible to determine whether the block is type I or
of block is often permanent and progresses to complete block. Ex- II without intracardiac recordings. However, an educated guess
ternal pacing can be used for the treatment of symptomatic type II can be made depending on the length of the PR interval, the QRS
block until transvenous pacing can be initiated. Atropine is not rec- width, and the clinical situation. The following ECG findings can
ommended because it may result in further slowing of ventricular be very helpful in determining the type of block in 2:1 conduc-
rate by increasing the number of impulses conducting through the tion in the absence of intracardiac recordings:
AV node and bombarding the diseased bundles with more impulses PR interval: Often longer than normal (more than 0.20 sec-
than they can handle, resulting in further conduction failure. ond) in type I and normal in type II. Sometimes, the PR in
A A
B B
Examples of 2:1 conduction