
Page 704 - Cardiac Nursing
P. 704
5-7
04.
qxd
p65
680
tar
Ap
AM
P
g
49
7
/1/
09
K34
0-c
28_
LWB K34 0-c 28_ p65 5-7 04. qxd 7 /1/ 09 9: 49 AM P a a g e e 680 Ap tar a a
LWB
LWBK340-c28_p655-704.qxd 7/1/09 9:9:49 AM Page 680 Aptara
680 PA R T I V / Pathophysiology and Management Disease
A
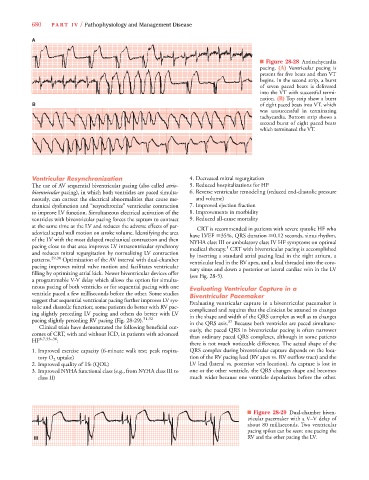
■ Figure 28-28 Antitachycardia
pacing. (A) Ventricular pacing is
present for five beats and then VT
begins. In the second strip, a burst
of seven paced beats is delivered
into the VT with successful termi-
nation. (B) Top strip show a burst
B of eight paced beats into VT, which
was unsuccessful in terminating
tachycardia. Bottom strip shows a
second burst of eight paced beats
which terminated the VT.
Ventricular Resynchronization 4. Decreased mitral regurgitation
The use of AV sequential biventricular pacing (also called atrio- 5.Reduced hospitalizations for HF
biventricular pacing), in which both ventricles are paced simulta- 6. Reverse ventricular remodeling (reduced end-diastolic pressure
neously, can correct the electrical abnormalities that cause me- and volume)
chanical dysfunction and “resynchronize” ventricular contraction 7. Improved ejection fraction
to improve LV function. Simultaneous electrical activation of the 8. Improvements in morbidity
ventricles with biventricular pacing forces the septum to contract 9. Reduced all-cause mortality
at the same time as the LV and reduces the adverse effects of par- CRT is recommended in patients with severe systolic HF who
adoxical septal wall motion on stroke volume. Identifying the area have LVEF 35%, QRS duration 0.12 seconds, sinus rhythm,
of the LV with the most delayed mechanical contraction and then NYHA class III or ambulatory class IV HF symptoms on optimal
pacing close to that area improves LV intraventricular synchrony medical therapy. CRT with biventricular pacing is accomplished
1
and reduces mitral regurgitation by normalizing LV contraction by inserting a standard atrial pacing lead in the right atrium, a
patterns. 29,30 Optimization of the AV interval with dual-chamber ventricular lead in the RV apex, and a lead threaded into the coro-
pacing improves mitral valve motion and facilitates ventricular nary sinus and down a posterior or lateral cardiac vein in the LV
filling by optimizing atrial kick. Newer biventricular devices offer (see Fig. 28-5).
a programmable V-V delay which allows the option for simulta-
neous pacing of both ventricles or for sequential pacing with one Evaluating Ventricular Capture in a
ventricle paced a few milliseconds before the other. Some studies Biventricular Pacemaker
suggest that sequential ventricular pacing further improves LV sys- Evaluating ventricular capture in a biventricular pacemaker is
tolic and diastolic function; some patients do better with RV pac- complicated and requires that the clinician be attuned to changes
ing slightly preceding LV pacing and others do better with LV in the shape and width of the QRS complex as well as to changes
pacing slightly preceding RV pacing (Fig. 28-29). 31,32 in the QRS axis. 37 Because both ventricles are paced simultane-
Clinical trials have demonstrated the following beneficial out- ously, the paced QRS in biventricular pacing is often narrower
comes of CRT, with and without ICD, in patients with advanced than ordinary paced QRS complexes, although in some patients
HF 6,7,33–36 :
there is not much noticeable difference. The actual shape of the
1. Improved exercise capacity (6-minute walk test; peak respira- QRS complex during biventricular capture depends on the loca-
tory O 2 uptake) tion of the RV pacing lead (RV apex vs. RV outflow tract) and the
2. Improved quality of life (QOL) LV lead (lateral vs. posterior vein location). As capture is lost in
3. Improved NYHA functional class (e.g., from NYHA class III to one or the other ventricle, the QRS changes shape and becomes
class II) much wider because one ventricle depolarizes before the other.
■ Figure 28-29 Dual-chamber biven-
tricular pacemaker with a V–V delay of
about 80 milliseconds. Two ventricular
pacing spikes can be seen: one pacing the
I I II II II RV and the other pacing the LV.