
Page 701 - Cardiac Nursing
P. 701
92806_c28.qxd 11/21/11 11:03 AM Page 677
C H A P T E R 2 8 / Pacemakers and Implantable Defibrillators 677
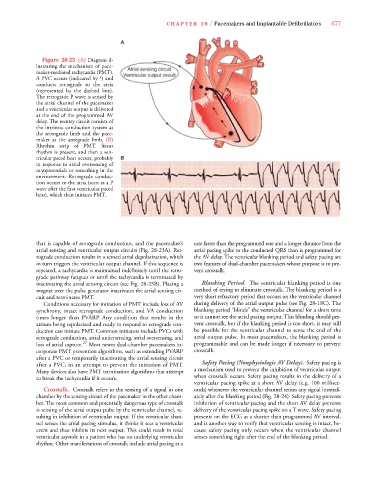
F i g u re 28-23 ( A ) Diagram il-
lustrating the mechanism of pace-
maker-mediated tachyc a rdia (PMT) .
A PVC occurs (indicated by *) and
conducts re t rograde to the atria
( re p resented by the dashed line).
The retrograde P wave is sensed by
the atrial channel of the pacemaker
and a ventricular output is delivered
at the end of the programmed AV
delay. The reentry circuit consists of
the intrinsic conduction system as
the re t rograde limb and the pace-
maker as the antegrade limb. ( B )
Rhythm strip of PMT. Si n u s
rhythm is present, and then a ve n-
tricular paced beat occurs, probably
in response to atrial oversensing of
m yopotentials or something in the
e n v i ronment. Re t rograde conduc-
tion occurs to the atria (seen as a P
wave after the first ventricular paced
beat), which then initiates PMT.
that is capable of re t rograde conduction, and the pacemaker’s rate faster than the programmed rate and a longer distance from the
atrial sensing and ventricular output circuits (Fig. 28-23A). Ret- atrial pacing spike to the conducted QRS than is programmed for
rograde conduction results in a sensed atrial depolarization, which the AV delay. The ventricular blanking period and safety pacing are
in turn triggers the ventricular output channel. If this sequence is two features of dual-chamber pacemakers whose purpose is to pre-
repeated, a tachycardia is maintained indefinitely until the retro- vent cro s s t a l k .
grade pathway fatigues or until the tachycardia is terminated by
inactivating the atrial sensing circuit (see Fig. 28-23B). Placing a Blanking Pe r i o d . The ventricular blanking period is one
magnet over the pulse generator inactivates the atrial sensing cir- method of trying to eliminate crosstalk. The blanking period is a
cuit and terminates PMT. very short refractory period that occurs on the ventricular channel
Conditions necessary for initiation of PMT include loss of AV during delivery of the atrial output pulse (see Fig. 28-18C). The
s y n c h ro n y, intact re t rograde conduction, and VA conduction blanking period “blinds” the ventricular channel for a short time
times longer than PVA R P. Any condition that results in the so it cannot see the atrial pacing output. This blinding should pre-
atrium being repolarized and ready to respond to retrograde con- vent crosstalk, but if the blanking period is too short, it may still
duction can initiate PMT. Common initiators include PVCs with be possible for the ventricular channel to sense the end of the
retrograde conduction, atrial undersensing, atrial oversensing, and atrial output pulse. In most pacemakers, the blanking period is
loss of atrial capture. 27 Most newer dual-chamber pacemakers in- p rogrammable and can be made longer if necessary to pre ve n t
corporate PMT prevention algorithms, such as extending PVARP crosstalk.
after a PVC or temporarily inactivating the atrial sensing circuit
after a PVC, in an attempt to pre vent the initiation of PMT. Safety Pacing (Nonphysiologic AV Delay). Safety pacing is
Many devices also have PMT termination algorithms that attempt a mechanism used to prevent the inhibition of ventricular output
to break the tachycardia if it occurs. when crosstalk occurs. Safety pacing results in the delive ry of a
ventricular pacing spike at a short AV delay (e.g. 100 millisec-
Cro s s t a l k . Crosstalk refers to the sensing of a signal in one onds) whenever the ventricular channel senses any signal immedi-
chamber by the sensing circuit of the pacemaker in the other cham- ately after the blanking period (Fig. 28-24). Safety pacing prevents
b e r. The most common and potentially dangerous type of cro s s t a l k inhibition of ventricular pacing and the short AV delay prevents
is sensing of the atrial output pulse by the ventricular channel, re- delivery of the ventricular pacing spike on a T wave. Safety pacing
sulting in inhibition of ventricular output. If the ventricular chan- presents on the ECG as a shorter than programmed AV interval,
nel senses the atrial pacing stimulus, it thinks it sees a ve n t r i c u l a r and is another way to verify that ventricular sensing is intact, be-
e vent and thus inhibits its next output. This could result in total cause safety pacing only occurs when the ventricular channel
ventricular asystole in a patient who has no underlying ve n t r i c u l a r senses something right after the end of the blanking period.
rhythm. Other manifestations of crosstalk include atrial pacing at a