
Page 617 - Williams Hematology ( PDFDrive )
P. 617
592 Part VI: The Erythrocyte Chapter 41: Folate, Cobalamin, and Megaloblastic Anemias 593
OH OH OH OH
O O
N N N N
CN
5 N 5 N
OH CH 2 N CH 2 N
NH NH OH
O 2 Coenzyme 2
synthetase
Co + P Co + P P P
P
P
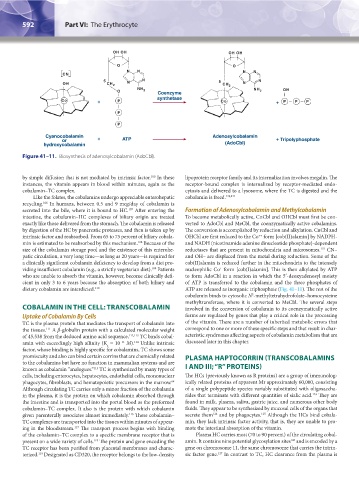
Cyanocobalamin Adenosylcobalamin
or + ATP + Tripolyphosphate
hydroxycobalamin (AdoCbl)
Figure 41–11. Biosynthesis of adenosylcobalamin (AdoCbl).
by simple diffusion that is not mediated by intrinsic factor. In these lipoprotein receptor family and its internalization involves megalin. The
100
instances, the vitamin appears in blood within minutes, again as the receptor-bound complex is internalized by receptor-mediated endo-
cobalamin–TC complex. cytosis and delivered to a lysosome, where the TC is digested and the
Like the folates, the cobalamins undergo appreciable enterohepatic cobalamin is freed. 120,121
recycling. In humans, between 0.5 and 9 mcg/day of cobalamin is
106
secreted into the bile, where it is bound to HC. After entering the Formation of Adenosylcobalamin and Methylcobalamin
107
intestine, the cobalamin–HC complexes of biliary origin are treated To become metabolically active, CnCbl and OHCbl must first be con-
exactly like those delivered from the stomach. The cobalamin is released verted to AdoCbl and MeCbl, the coenzymatically active cobalamins.
by digestion of the HC by pancreatic proteases, and then is taken up by The conversion is accomplished by reduction and alkylation. CnCbl and
intrinsic factor and reabsorbed. From 65 to 75 percent of biliary cobala- OHCbl are first reduced to the Co form [cob(II)alamin] by NADPH-
++
min is estimated to be reabsorbed by this mechanism. Because of the and NADH (nicotinamide adenine dinucleotide phosphate)-dependent
108
size of the cobalamin storage pool and the existence of this enterohe- reductases that are present in mitochondria and microsomes. CN–
122
patic circulation, a very long time—as long as 20 years—is required for and OH– are displaced from the metal during reduction. Some of the
a clinically significant cobalamin deficiency to develop from a diet pro- cob(II)alamin is reduced further in the mitochondria to the intensely
viding insufficient cobalamin (e.g., a strictly vegetarian diet). Patients nucleophilic Co form [cob(I)alamin]. This is then alkylated by ATP
+
109
who are unable to absorb the vitamin, however, become clinically defi- to form AdoCbl in a reaction in which the 5′-deoxyadenosyl moiety
cient in only 3 to 6 years because the absorption of both biliary and of ATP is transferred to the cobalamin and the three phosphates of
dietary cobalamin are interdicted. 110 ATP are released as inorganic triphosphate (Fig. 41–11). The rest of the
cobalamin binds to cytosolic N -methyltetrahydrofolate–homocysteine
5
methyltransferase, where it is converted to MeCbl. The several steps
COBALAMIN IN THE CELL: TRANSCOBALAMIN involved in the conversion of cobalamin to its coenzymatically active
Uptake of Cobalamin By Cells forms are regulated by genes that play a critical role in the processing
TC is the plasma protein that mediates the transport of cobalamin into of the vitamin. There are a number of inherited metabolic errors that
the tissues. A β-globulin protein with a calculated molecular weight correspond to one or more of these specific steps and that result in char-
111
of 45,538 from the deduced amino acid sequence, 112,113 TC binds cobal- acteristic syndromes affecting aspects of cobalamin metabolism that are
amin with exceedingly high affinity (K = 10 M). Unlike intrinsic discussed later in this chapter.
–11
114
a
factor, whose binding is highly specific for cobalamins, TC shows some
promiscuity and also can bind certain corrins that are chemically related PLASMA HAPTOCORRIN (TRANSCOBALAMINS
to the cobalamins but have no function in mammalian systems and are
known as cobalamin “analogues.” TC is synthesized by many types of I AND III; “R” PROTEINS)
115
cells, including enterocytes, hepatocytes, endothelial cells, mononuclear The HCs (previously known as R proteins) are a group of immunolog-
phagocytes, fibroblasts, and hematopoietic precursors in the marrow. ically related proteins of apparent Mr approximately 60,000, consisting
64
Although circulating TC carries only a minor fraction of the cobalamin of a single polypeptide species variably substituted with oligosaccha-
in the plasma, it is the protein on which cobalamin absorbed through rides that terminate with different quantities of sialic acid. They are
123
the intestine and is transported into the portal blood as the preformed found in milk, plasma, saliva, gastric juice, and numerous other body
cobalamin–TC complex. It also is the protein with which cobalamin fluids. They appear to be synthesized by mucosal cells of the organs that
124
given parenterally associates almost immediately. These cobalamin– secrete them and by phagocytes. Although the HCs bind cobala-
125
116
TC complexes are transported into the tissues within minutes of appear- min, they lack intrinsic factor activity, that is, they are unable to pro-
ing in the bloodstream. The transport process begins with binding mote the intestinal absorption of the vitamin.
117
of the cobalamin–TC complex to a specific membrane receptor that is Plasma HC carries most (70 to 90 percent) of the circulating cobal-
present on a wide variety of cells. The protein and gene encoding the amin. It contains nine potential glycosylation sites and is encoded by a
126
118
TC receptor has been purified from placental membranes and charac- gene on chromosome 11, the same chromosome that carries the intrin-
terized. Designated as CD320, the receptor belongs to the low-density sic factor gene. In contrast to TC, HC clearance from the plasma is
127
119
Kaushansky_chapter 41_p0583-0616.indd 592 9/17/15 6:24 PM