
Page 1385 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1385
958 PART 8: Renal and Metabolic Disorders
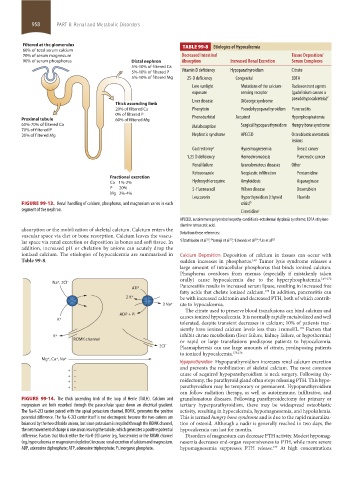
Filtered at the glomerulus TABLE 99-8 Etiologies of Hypocalcemia
60% of total serum calcium
70% of serum magnesium Decreased Intestinal Tissue Deposition/
90% of serum phosphorus Distal nephron Absorption Increased Renal Excretion Serum Complexes
5%-10% of filtered Ca
5%-10% of filtered P Vitamin D deficiency Hypoparathyroidism Citrate
5%-10% of filtered Mg 25-D deficiency Congenital EDTA
Low sunlight Mutations of the calcium- Radiocontrast agents
exposure sensing receptor (gadolinium causes a
Liver disease DiGeorge syndrome pseudohypocalcemia) d
Thick ascending limb
20% of filtered Ca Phenytoin Pseudohypoparathyroidism Pancreatitis
0% of filtered P Phenobarbital Acquired Hyperphosphatemia
Proximal tubule 60% of filtered Mg
60%-70% of filtered Ca Malabsorption Surgical hypoparathyroidism Hungry bone syndrome
70% of filtered P
30% of filtered Mg Nephrotic syndrome APECED Osteoblastic metastatic
lesions
Gastrectomy a Hypermagnesemia Breast cancer
1,25 D deficiency Hemochromatosis Pancreatic cancer
Renal failure Granulomatous diseases Other
Ketoconazole Neoplastic infiltration Pentamidine
Fractional excretion
Ca 1%-2% Hydroxychloroquine Amyloidosis Asparaginase
P 20% 5-Fluorouracil Wilson disease Doxorubicin
Mg 2%-4%
Leucovorin Hyperthyroidism (thyroid Fluoride
FIGURE 99-13. Renal handling of calcium, phosphorus, and magnesium varies in each crisis) b
segment of the nephron. Cimetidine c
APECED, autoimmune polyendocrinopathy-candidiasis-ectodermal dysplasia syndrome; EDTA ethylene-
diamine tetraacetic acid.
absorption or the mobilization of skeletal calcium. Calcium enters the
vascular space via diet or bone resorption. Calcium leaves the vascu- Data from these references:
323 c
325
324 d
322 b
lar space via renal excretion or deposition in bones and soft tissue. In a Efstathiadou et al ; Yamaji et al ; Edwards et al ; Lin et al
addition, increased pH or chelation by anions can acutely drop the
ionized calcium. The etiologies of hypocalcemia are summarized in Calcium Deposition Deposition of calcium in tissues can occur with
Table 99-8. sudden increases in phosphorus. Tumor lysis syndrome releases a
169
large amount of intracellular phosphorus that binds ionized calcium.
Phosphorus overdoses from enemas (especially if mistakenly taken
orally) cause hypocalcemia due to the hyperphosphatemia. 169-172
Na + , 2CI – Pancreatitis results in increased serum lipase, resulting in increased free
ATP
fatty acids that chelate ionized calcium. In addition, pancreatitis can
173
2 K + be with increased calcitonin and decreased PTH, both of which contrib-
3 Na + ute to hypocalcemia.
The citrate used to preserve blood transfusions can bind calcium and
ADP + Pi causes ionized hypocalcemia. It is normally rapidly metabolized and well
K +
tolerated, despite transient decreases in calcium; 10% of patients tran-
siently have ionized calcium levels less than 1 mmol/L. Factors that
174
K + inhibit citrate metabolism (liver failure, kidney failure, or hypothermia)
ROMK channel or rapid or large transfusions predispose patients to hypocalcemia.
2CI – Plasmapheresis can use large amounts of citrate, predisposing patients
to ionized hypocalcemia. 175,176
Mg + , Ca + , Na +
Hypoparathyroidism Hypoparathyroidism increases renal calcium excretion
and prevents the mobilization of skeletal calcium. The most common
+ –
+ – cause of acquired hypoparathyroidism is neck surgery. Following thy-
+ – roidectomy, the parathyroid gland often stops releasing PTH. This hypo-
+ – parathyroidism may be temporary or permanent. Hypoparathyroidism
can follow radiation therapy, as well as autoimmune, infiltrative, and
FIGURE 99-14. The thick ascending limb of the loop of Henle (TALH). Calcium and granulomatous diseases. Following parathyroidectomy for primary or
magnesium are both resorbed through the paracellular space down an electrical gradient. tertiary hyperparathyroidism, there may be widespread osteoblastic
The Na-K-2Cl carrier paired with the apical potassium channel, ROMK, generates the positive activity, resulting in hypocalcemia, hypomagnesemia, and hypokalemia.
potential difference. The Na-K-2Cl carrier itself is not electrogenic because the two cations are This is termed hungry bone syndrome and is due to the rapid mineraliza-
balanced by the two chloride anions, but since potassium is recycled through the ROMK channel, tion of osteoid. Although a nadir is generally reached in two days, the
the net movement of charge is one anion leaving the tubule, which generates a positive potential hypocalcemia can last for months.
difference. Factors that block either the Na-K-2Cl carrier (eg, furosemide) or the ROMK channel Disorders of magnesium can decrease PTH activity. Modest hypomag-
(eg, hypercalcemia or magnesium depletion) increase renal excretion of calcium and magnesium. nesemia decreases end-organ responsiveness to PTH, while more severe
ADP, adenosine diphosphate; ATP, adenosine triphosphate; Pi, inorganic phosphate. hypomagnesemia suppresses PTH release. At high concentrations
177
section08.indd 958 1/14/2015 8:28:19 AM