
Page 344 - Textbook of Pathology, 6th Edition
P. 344
328
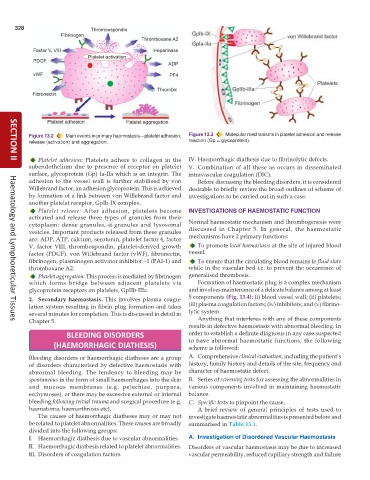
Figure 13.2 Main events in primary haemostasis—platelet adhesion, Figure 13.3 Molecular mechanisms in platelet adhesion and release
release (activation) and aggregation. reaction (Gp = glycoprotein).
Platelet adhesion: Platelets adhere to collagen in the IV. Haemorrhagic diathesis due to fibrinolytic defects.
SECTION II
subendothelium due to presence of receptor on platelet V. Combination of all these as occurs in disseminated
surface, glycoprotein (Gp) Ia-IIa which is an integrin. The intravascular coagulation (DIC).
adhesion to the vessel wall is further stabilised by von Before discussing the bleeding disorders, it is considered
Willebrand factor, an adhesion glycoprotein. This is achieved desirable to briefly review the broad outlines of scheme of
by formation of a link between von Willebrand factor and investigations to be carried out in such a case.
another platelet receptor, GpIb-IX complex.
Platelet release: After adhesion, platelets become INVESTIGATIONS OF HAEMOSTATIC FUNCTION
activated and release three types of granules from their
cytoplasm: dense granules, α-granules and lysosomal Normal haemostatic mechanism and thrombogenesis were
vesicles. Important products released from these granules discussed in Chapter 5. In general, the haemostatic
are: ADP, ATP, calcium, serotonin, platelet factor 4, factor mechanisms have 2 primary functions:
V, factor VIII, thrombospondin, platelet-derived growth To promote local haemostasis at the site of injured blood
factor (PDGF), von Willebrand factor (vWF), fibronectin, vessel.
fibrinogen, plasminogen activator inhibitor –1 (PAI-1) and To ensure that the circulating blood remains in fluid state
thromboxane A2. while in the vascular bed i.e. to prevent the occurrence of
Platelet aggregation: This process is mediated by fibrinogen generalised thrombosis.
which forms bridge between adjacent platelets via Formation of haemostatic plug is a complex mechanism
glycoprotein receptors on platelets, GpIIb-IIIa. and involves maintenance of a delicate balance among at least
2. Secondary haemostasis. This involves plasma coagu- 5 components (Fig. 13.4): (i) blood vessel wall; (ii) platelets;
lation system resulting in fibrin plug formation and takes (iii) plasma coagulation factors; (iv) inhibitors; and (v) fibrino-
several minutes for completion. This is discussed in detail in lytic system.
Chapter 5. Anything that interferes with any of these components
Haematology and Lymphoreticular Tissues
results in defective haemostasis with abnormal bleeding. In
BLEEDING DISORDERS order to establish a definite diagnosis in any case suspected
to have abnormal haemostatic functions, the following
(HAEMORRHAGIC DIATHESIS) scheme is followed:
Bleeding disorders or haemorrhagic diatheses are a group A. Comprehensive clinical evaluation, including the patient’s
of disorders characterised by defective haemostasis with history, family history and details of the site, frequency and
abnormal bleeding. The tendency to bleeding may be character of haemostatic defect.
spontaneous in the form of small haemorrhages into the skin B. Series of screening tests for assessing the abnormalities in
and mucous membranes (e.g. petechiae, purpura, various components involved in maintaining haemostatic
ecchymoses), or there may be excessive external or internal balance.
bleeding following trivial trauma and surgical procedure (e.g. C. Specific tests to pinpoint the cause.
haematoma, haemarthrosis etc). A brief review of general principles of tests used to
The causes of haemorrhagic diatheses may or may not investigate haemostatic abnormalities is presented below and
be related to platelet abnormalities. These causes are broadly summarised in Table 13.1.
divided into the following groups:
I. Haemorrhagic diathesis due to vascular abnormalities. A. Investigation of Disordered Vascular Haemostasis
II. Haemorrhagic diathesis related to platelet abnormalities. Disorders of vascular haemostasis may be due to increased
III. Disorders of coagulation factors. vascular permeability, reduced capillary strength and failure