
Page 451 - Textbook of Pathology, 6th Edition
P. 451
435
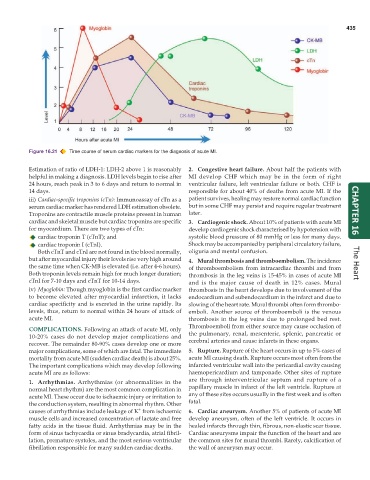
Figure 16.21 Time course of serum cardiac markers for the diagnosis of acute MI.
Estimation of ratio of LDH-1: LDH-2 above 1 is reasonably 2. Congestive heart failure. About half the patients with
helpful in making a diagnosis. LDH levels begin to rise after MI develop CHF which may be in the form of right
24 hours, reach peak in 3 to 6 days and return to normal in ventricular failure, left ventricular failure or both. CHF is
14 days. responsible for about 40% of deaths from acute MI. If the
iii) Cardiac-specific troponins (cTn): Immunoassay of cTn as a patient survives, healing may restore normal cardiac function
serum cardiac marker has rendered LDH estimation obsolete. but in some CHF may persist and require regular treatment
Troponins are contractile muscle proteins present in human later. CHAPTER 16
cardiac and skeletal muscle but cardiac troponins are specific 3. Cardiogenic shock. About 10% of patients with acute MI
for myocardium. There are two types of cTn: develop cardiogenic shock characterised by hypotension with
cardiac troponin T (cTnT); and systolic blood pressure of 80 mmHg or less for many days.
cardiac troponin I (cTnI). Shock may be accompanied by peripheral circulatory failure,
Both cTnT and cTnI are not found in the blood normally, oliguria and mental confusion.
but after myocardial injury their levels rise very high around 4. Mural thrombosis and thromboembolism. The incidence
the same time when CK-MB is elevated (i.e. after 4-6 hours). of thromboembolism from intracardiac thrombi and from The Heart
Both troponin levels remain high for much longer duration; thrombosis in the leg veins is 15-45% in cases of acute MI
cTnI for 7-10 days and cTnT for 10-14 days. and is the major cause of death in 12% cases. Mural
iv) Myoglobin: Though myoglobin is the first cardiac marker thrombosis in the heart develops due to involvement of the
to become elevated after myocardial infarction, it lacks endocardium and subendocardium in the infarct and due to
cardiac specificity and is excreted in the urine rapidly. Its slowing of the heart rate. Mural thrombi often form thrombo-
levels, thus, return to normal within 24 hours of attack of emboli. Another source of thromboemboli is the venous
acute MI. thrombosis in the leg veins due to prolonged bed rest.
Thromboemboli from either source may cause occlusion of
COMPLICATIONS. Following an attack of acute MI, only
10-20% cases do not develop major complications and the pulmonary, renal, mesenteric, splenic, pancreatic or
recover. The remainder 80-90% cases develop one or more cerebral arteries and cause infarcts in these organs.
major complications, some of which are fatal. The immediate 5. Rupture. Rupture of the heart occurs in up to 5% cases of
mortality from acute MI (sudden cardiac death) is about 25%. acute MI causing death. Rupture occurs most often from the
The important complications which may develop following infarcted ventricular wall into the pericardial cavity causing
acute MI are as follows: haemopericardium and tamponade. Other sites of rupture
are through interventricular septum and rupture of a
1. Arrhythmias. Arrhythmias (or abnormalities in the
normal heart rhythm) are the most common complication in papillary muscle in infarct of the left ventricle. Rupture at
acute MI. These occur due to ischaemic injury or irritation to any of these sites occurs usually in the first week and is often
the conduction system, resulting in abnormal rhythm. Other fatal.
+
causes of arrhythmias include leakage of K from ischaemic 6. Cardiac aneurysm. Another 5% of patients of acute MI
muscle cells and increased concentration of lactate and free develop aneurysm, often of the left ventricle. It occurs in
fatty acids in the tissue fluid. Arrhythmias may be in the healed infarcts through thin, fibrous, non-elastic scar tissue.
form of sinus tachycardia or sinus bradycardia, atrial fibril- Cardiac aneurysms impair the function of the heart and are
lation, premature systoles, and the most serious ventricular the common sites for mural thrombi. Rarely, calcification of
fibrillation responsible for many sudden cardiac deaths. the wall of aneurysm may occur.