
Page 637 - Textbook of Pathology, 6th Edition
P. 637
occurrence of gout, impaired gluconeogenesis and altered 621
steroid metabolism.
8. Retention of liver cell water and proteins. Alcohol is
inhibitory to secretion of newly-synthesised proteins by the
liver leading to their retention in the hepatocytes. Water is
simultaneously retained in the cell in proportion to the
protein and results in swelling of hepatocytes resulting in
hepatomegaly in alcoholics.
9. Hypoxia. Chronic ingestion of alcohol results in increased
oxygen demand by the liver resulting in a hypoxic state
which causes hepatocellular necrosis in centrilobular zone
(zone 3). Redox changes are also more marked in zone 3.
10. Increased liver fat. The origin of fat in the body was
discussed in Chapter 3 (page 37). In chronic alcoholism, there
is rise in the amount of fat available to the liver which could
be from exogenous (dietary) sources, excess mobilisation
from adipose tissue or increased lipid synthesis by the liver
itself. This may account for lipid accumulation in the
hepatocytes.
MORPHOLOGIC FEATURES. Three types of morpho-
logic lesions are described in alcoholic liver disease—
alcoholic steatosis (fatty liver), alcoholic hepatitis and
alcoholic cirrhosis.
1. ALCOHOLIC STEATOSIS (FATTY LIVER). The CHAPTER 21
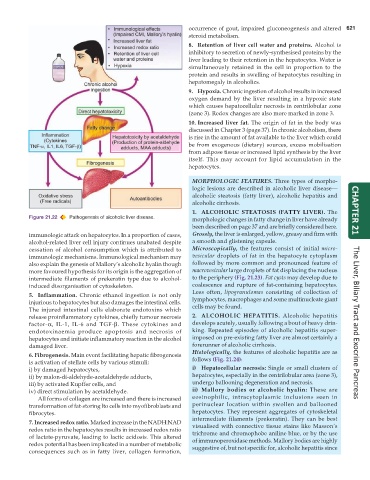
Figure 21.22 Pathogenesis of alcoholic liver disease. morphologic changes in fatty change in liver have already
been described on page 37 and are briefly considered here.
immunologic attack on hepatocytes. In a proportion of cases, Grossly, the liver is enlarged, yellow, greasy and firm with
alcohol-related liver cell injury continues unabated despite a smooth and glistening capsule.
cessation of alcohol consumption which is attributed to Microscopically, the features consist of initial micro-
immunologic mechanisms. Immunological mechanism may vesicular droplets of fat in the hepatocyte cytoplasm
also explain the genesis of Mallory’s alcoholic hyalin though followed by more common and pronounced feature of
more favoured hypothesis for its origin is the aggregation of macrovesicular large droplets of fat displacing the nucleus
intermediate filaments of prekeratin type due to alcohol- to the periphery (Fig. 21.23). Fat cysts may develop due to
induced disorganisation of cytoskeleton. coalescence and rupture of fat-containing hepatocytes.
Less often, lipogranulomas consisting of collection of
5. Inflammation. Chronic ethanol ingestion is not only
injurious to hepatocytes but also damages the intestinal cells. lymphocytes, macrophages and some multinucleate giant
The injured intestinal cells elaborate endotoxins which cells may be found.
release proinflammatory cytokines, chiefly tumour necrosis 2. ALCOHOLIC HEPATITIS. Alcoholic hepatitis
factor-α, IL-1, IL-6 and TGF-β. These cytokines and develops acutely, usually following a bout of heavy drin- The Liver, Biliary Tract and Exocrine Pancreas
endotoxinaemia produce apoptosis and necrosis of king. Repeated episodes of alcoholic hepatitis super-
hepatocytes and initiate inflammatory reaction in the alcohol imposed on pre-existing fatty liver are almost certainly a
damaged liver. forerunner of alcoholic cirrhosis.
Histologically, the features of alcoholic hepatitis are as
6. Fibrogenesis. Main event facilitating hepatic fibrogenesis
is activation of stellate cells by various stimuli: follows (Fig. 21.24):
i) by damaged hepatocytes, i) Hepatocellular necrosis: Single or small clusters of
ii) by malon-di-aldehyde-acetaldehyde adducts, hepatocytes, especially in the centrilobular area (zone 3),
iii) by activated Kupffer cells, and undergo ballooning degeneration and necrosis.
iv) direct stimulation by acetaldehyde. ii) Mallory bodies or alcoholic hyalin: These are
All forms of collagen are increased and there is increased eosinophilic, intracytoplasmic inclusions seen in
transformation of fat-storing lto cells into myofibroblasts and perinuclear location within swollen and ballooned
fibrocytes. hepatocytes. They represent aggregates of cytoskeletal
intermediate filaments (prekeratin). They can be best
7. Increased redox ratio. Marked increase in the NADH:NAD visualised with connective tissue stains like Masson’s
redox ratio in the hepatocytes results in increased redox ratio trichrome and chromophobe aniline blue, or by the use
of lactate-pyruvate, leading to lactic acidosis. This altered of immunoperoxidase methods. Mallory bodies are highly
redox potential has been implicated in a number of metabolic suggestive of, but not specific for, alcoholic hepatitis since
consequences such as in fatty liver, collagen formation,