
Page 725 - First Aid for the USMLE Step 1 2020, Thirtieth edition [MedicalBooksVN.com]_Neat
P. 725
RespiRatoRy ` RESPIRATORY—PAThOlOgY RespiRatoRy ` RESPIRATORY—PAThOlOgY seCtioN iii 681
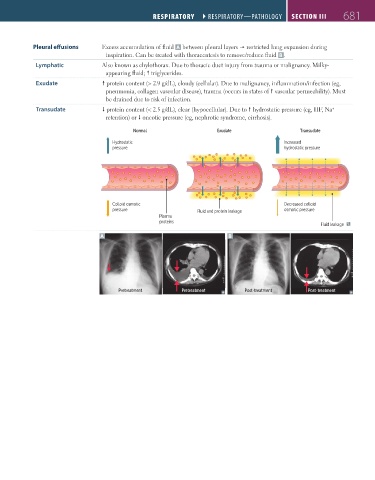
Pleural effusions Excess accumulation of fluid A between pleural layers restricted lung expansion during
inspiration. Can be treated with thoracentesis to remove/reduce fluid B .
Lymphatic Also known as chylothorax. Due to thoracic duct injury from trauma or malignancy. Milky-
appearing fluid; triglycerides.
Exudate protein content (> 2.9 g/dL), cloudy (cellular). Due to malignancy, inflammation/infection (eg,
pneumonia, collagen vascular disease), trauma (occurs in states of vascular permeability). Must
be drained due to risk of infection.
Transudate protein content (< 2.5 g/dL), clear (hypocellular). Due to hydrostatic pressure (eg, HF, Na
+
retention) or oncotic pressure (eg, nephrotic syndrome, cirrhosis).
Normal Exudate Transudate
Hydrostatic Increased
pressure hydrostatic pressure
Colloid osmotic Decreased colloid
pressure Fluid and protein leakage osmotic pressure
Plasma
proteins
Fluid leakage
A B
Pretreatment Pretreatment Post-treatment Post-treatment
FAS1_2019_16-Respiratory.indd 681 11/8/19 7:34 AM