
Page 111 - The Netter Collection of Medical Illustrations - Integumentary System_ Volume 4 ( PDFDrive )
P. 111
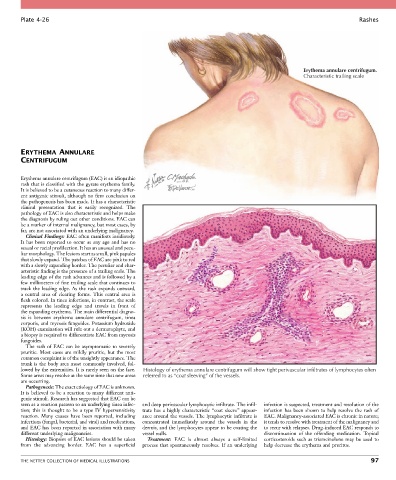
Plate 4-26 Rashes
Erythema annulare centrifugum.
Characteristic trailing scale
ERYTHEMA ANNULARE
CENTRIFUGUM
Erythema annulare centrifugum (EAC) is an idiopathic
rash that is classified with the gyrate erythema family.
It is believed to be a cutaneous reaction to many differ-
ent antigenic stimuli, although no firm conclusion on
the pathogenesis has been made. It has a characteristic
clinical presentation that is easily recognized. The
pathology of EAC is also characteristic and helps make
the diagnosis by ruling out other conditions. EAC can
be a marker of internal malignancy, but most cases, by
far, are not associated with an underlying malignancy.
Clinical Findings: EAC often manifests insidiously.
It has been reported to occur at any age and has no
sexual or racial predilection. It has an unusual and pecu-
liar morphology. The lesions start as small, pink papules
that slowly expand. The patches of EAC are pink to red
with a slowly expanding border. The peculiar and char-
acteristic finding is the presence of a trailing scale. The
leading edge of the rash advances and is followed by a
few millimeters of fine trailing scale that continues to
track the leading edge. As the rash expands outward,
a central area of clearing forms. This central area is
flesh colored. In tinea infections, in contrast, the scale
represents the leading edge and travels in front of
the expanding erythema. The main differential diagno-
sis is between erythema annulare centrifugum, tinea
corporis, and mycosis fungoides. Potassium hydroxide
(KOH) examination will rule out a dermatophyte, and
a biopsy is required to differentiate EAC from mycosis
fungoides.
The rash of EAC can be asymptomatic to severely
pruritic. Most cases are mildly pruritic, but the most
common complaint is of the unsightly appearance. The
trunk is the body area most commonly involved, fol-
lowed by the extremities. It is rarely seen on the face. Histology of erythema annulare centrifugum will show tight perivascular infiltrates of lymphocytes often
Some areas may resolve at the same time that new areas referred to as “coat sleeving” of the vessels.
are occurring.
Pathogenesis: The exact etiology of EAC is unknown.
It is believed to be a reaction to many different anti-
genic stimuli. Research has suggested that EAC can be
seen as a reaction pattern to an underlying tinea infec- and deep perivascular lymphocytic infiltrate. The infil- infection is suspected, treatment and resolution of the
tion; this is thought to be a type IV hypersensitivity trate has a highly characteristic “coat sleeve” appear- infection has been shown to help resolve the rash of
reaction. Many causes have been reported, including ance around the vessels. The lymphocytic infiltrate is EAC. Malignancy-associated EAC is chronic in nature;
infections (fungal, bacterial, and viral) and medications, concentrated immediately around the vessels in the it tends to resolve with treatment of the malignancy and
and EAC has been reported in association with many dermis, and the lymphocytes appear to be coating the to recur with relapses. Drug-induced EAC responds to
different underlying malignancies. vessel walls. discontinuation of the offending medication. Topical
Histology: Biopsies of EAC lesions should be taken Treatment: EAC is almost always a self-limited corticosteroids such as triamcinolone may be used to
from the advancing border. EAC has a superficial process that spontaneously resolves. If an underlying help decrease the erythema and pruritus.
THE NETTER COLLECTION OF MEDICAL ILLUSTRATIONS 97