
Page 155 - The Netter Collection of Medical Illustrations - Integumentary System_ Volume 4 ( PDFDrive )
P. 155
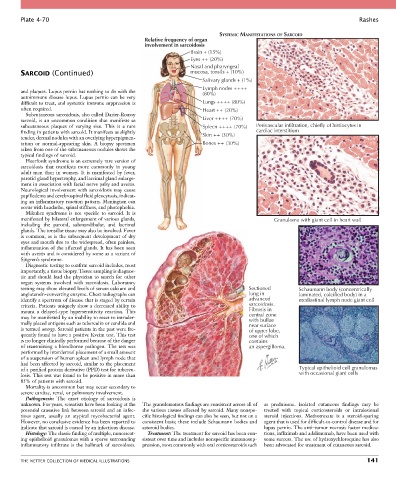
Plate 4-70 Rashes
SYSTEMIC MANIFESTATIONS OF SARCOID
Relative frequency of organ
involvement in sarcoidosis
Brain + (15%)
Eyes ++ (20%)
Nasal and pharyngeal
SARCOID (Continued) mucosa, tonsils + (10%)
Salivary glands + (1%)
Lymph nodes ++++
and plaques. Lupus pernio has nothing to do with the (80%)
autoimmune disease lupus. Lupus pernio can be very
difficult to treat, and systemic immune suppression is Lungs ++++ (80%)
often required. Heart ++ (20%)
Subcutaneous sarcoidosis, also called Darier-Roussy
sarcoid, is an uncommon condition that manifests as Liver ++++ (70%)
subcutaneous plaques of varying size. This is a rare Spleen ++++ (70%) Perivascular infiltration, chiefly of histiocytes in
finding in patients with sarcoid. It manifests as slightly Skin ++ (30%) cardiac interstitium
tender, dermal nodules with an overlying hyperpigmen-
tation or normal-appearing skin. A biopsy specimen Bones ++ (30%)
taken from one of the subcutaneous nodules shows the
typical findings of sarcoid.
Heerfordt syndrome is an extremely rare version of
sarcoidosis that manifests more commonly in young
adult men than in women. It is manifested by fever,
parotid gland hypertrophy, and lacrimal gland enlarge-
ment in association with facial nerve palsy and uveitis.
Neurological involvement with sarcoidosis may cause
papilledema and cerebrospinal fluid pleocytosis, indicat-
ing an inflammatory reaction pattern. Meningism can
occur with headache, spinal stiffness, and photophobia.
Mikulicz syndrome is not specific to sarcoid. It is
manifested by bilateral enlargement of various glands, Granuloma with giant cell in heart wall
including the parotid, submandibular, and lacrimal
glands. The tonsillar tissue may also be involved. Fever
is common, as is the subsequent development of dry
eyes and mouth due to the widespread, often painless,
inflammation of the affected glands. It has been seen
with uveitis and is considered by some as a variant of
Sjögren’s syndrome.
Diagnostic testing to confirm sarcoid includes, most
importantly, a tissue biopsy. Tissue sampling is diagnos-
tic and should lead the physician to search for other
organ systems involved with sarcoidosis. Laboratory
testing may show elevated levels of serum calcium and Sectioned Schaumann body (concentrically
angiotensin-converting enzyme. Chest radiographs can lung in laminated, calcified body) in a
identify a spectrum of disease that is staged by certain advanced mediastinal lymph node giant cell
criteria. Patients uniquely show a decreased ability to sarcoidosis.
mount a delayed-type hypersensitivity reaction. This Fibrosis in
may be manifested by an inability to react to intrader- central zone
with bullae
mally placed antigens such as tuberculin or candida and near surface
is termed anergy. Sarcoid patients in the past were fre- of upper lobe,
quently found to have a positive Kveim test. This test one of which
is no longer clinically performed because of the danger contains
of transmitting a bloodborne pathogen. The test was an aspergilloma.
performed by interdermal placement of a small amount
of a suspension of human spleen and lymph node that
had been affected by sarcoid, similar to the placement
of a purified protein derivative (PPD) test for tubercu- Typical epithelioid cell granulomas
losis. This test was found to be positive in more than with occasional giant cells
85% of patients with sarcoid.
Mortality is uncommon but may occur secondary to
severe cardiac, renal, or pulmonary involvement.
Pathogenesis: The exact etiology of sarcoidosis is
unknown. For years, scientists have been looking at the The granulomatous findings are consistent across all of as prednisone. Isolated cutaneous findings may be
potential causative link between sarcoid and an infec- the various tissues affected by sarcoid. Many nonspe- treated with topical corticosteroids or intralesional
tious agent, usually an atypical mycobacterial agent. cific histological findings can also be seen, but not on a steroid injections. Methotrexate is a steroid-sparing
However, no conclusive evidence has been reported to consistent basis; these include Schaumann bodies and agent that is used for difficult-to-control disease and for
indicate that sarcoid is caused by an infectious disease. asteroid bodies. lupus pernio. The anti–tumor necrosis factor medica-
Histology: The classic finding of multiple, noncaseat- Treatment: The treatment for sarcoid has been con- tions, infliximab and adalimumab, have been used with
ing epithelioid granulomas with a sparse surrounding sistent over time and includes nonspecific immunosup- some success. The use of hydroxychloroquine has also
inflammatory infiltrate is the hallmark of sarcoidosis. pression, most commonly with oral corticosteroids such been advocated for treatment of cutaneous sarcoid.
THE NETTER COLLECTION OF MEDICAL ILLUSTRATIONS 141