
Page 246 - The Netter Collection of Medical Illustrations - Integumentary System_ Volume 4 ( PDFDrive )
P. 246
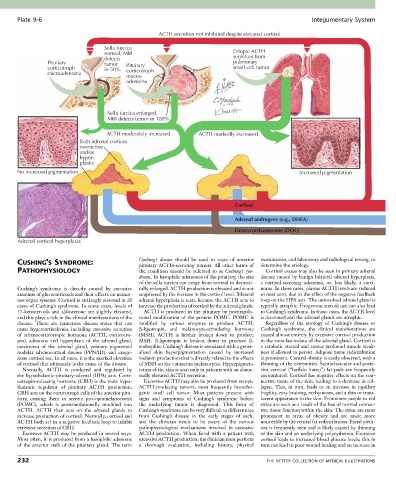
Plate 9-6 Integumentary System
ACTH secretion not inhibited despite elevated cortisol
Sella turcica
normal, MRI Ectopic ACTH
detects secretion from
Pituitary tumor Pituitary pulmonary
corticotroph in 50% corticotroph small cell tumor
microadenoma
macro-
adenoma
Sella turcica enlarged,
MRI detects tumor in 100%
ACTH moderately increased ACTH markedly increased
Both adrenal cortices
overactive
and/or
hyper-
plastic
No increased pigmentation Increased pigmentation
Cortisol
Adrenal androgens (e.g., DHEA)
Deoxycorticosterone (DOC)
Adrenal cortical hyperplasia
CUSHING’S SYNDROME: Cushing’s disease should be used in cases of anterior examination, and laboratory and radiological testing, to
pituitary ACTH-secreting tumors. All other forms of
determine the etiology.
PATHOPHYSIOLOGY the condition should be referred to as Cushing’s syn- Cortisol excess may also be seen in primary adrenal
drome. In basophilic adenomas of the pituitary, the size disease caused by benign bilateral adrenal hyperplasia,
of the sella turcica can range from normal to dramati- a cortisol-secreting adenoma, or, less likely, a carci-
Cushing’s syndrome is directly caused by excessive cally enlarged. ACTH production is elevated and is not noma. In these cases, plasma ACTH levels are reduced
amounts of glucocorticoids and their effects on numer- suppressed by the increase in the cortisol level. Bilateral to near zero, due to the effect of the negative feedback
ous organ systems. Cortisol is strikingly elevated in all adrenal hyperplasia is seen, because the ACTH acts to loop on the HPA axis. The uninvolved adrenal gland is
cases of Cushing’s syndrome. In some cases, levels of increase the production of cortisol by the adrenal glands. typically atrophic. Exogenous steroid use can also lead
17-ketosteroids and aldosterone are slightly elevated, ACTH is produced in the pituitary by posttransla- to Cushing’s syndrome. In those cases, the ACTH level
and this plays a role in the clinical manifestations of the tional modification of the protein POMC. POMC is is decreased and the adrenal glands are atrophic.
disease. There are numerous disease states that can modified by various enzymes to produce ACTH, Regardless of the etiology of Cushing’s disease or
cause hypercortisolemia, including excessive secretion β-lipotropin, and melanocyte-stimulating hormone Cushing’s syndrome, the clinical manifestations are
of adrenocorticotropic hormone (ACTH, corticotro- (MSH). ACTH is further broken down to produce caused almost entirely by excessive cortisol production
pin), adenoma and hyperplasia of the adrenal gland, MSH. β-lipotropin is broken down to produce β- in the zona fasciculata of the adrenal gland. Cortisol is
carcinoma of the adrenal gland, primary pigmented endorphin. Cushing’s disease is associated with a gener- a catabolic steroid and causes profound muscle weak-
nodular adrenocortical disease (PPNAD), and exoge- alized skin hyperpigmentation caused by increased ness if allowed to persist. Adipose tissue redistribution
nous cortisol use. In all cases, it is the marked elevation melanin production that is directly related to the effects is prominent. Central obesity is easily observed, with a
of cortisol that ultimately is the cause of the disease. of MSH on the cutaneous melanocytes. Hyperpigmen- thinning of the extremities. Supraclavicular and poste-
Normally, ACTH is produced and regulated by tation of the skin is seen only in patients with an abnor- rior cervical (“buffalo hump”) fat pads are frequently
the hypothalamic-pituitary-adrenal (HPA) axis. Corti- mally elevated ACTH secretion. encountered. Cortisol has negative effects on the con-
cotropin-releasing hormone (CRH) is the main hypo- Excessive ACTH may also be produced from ectopic nective tissue of the skin, leading to a decrease in col-
thalamic regulator of pituitary ACTH production. ACTH-producing tumors, most frequently broncho- lagen. This, in turn, leads to an increase in capillary
CRH acts on the corticotroph cells of the anterior pitu- genic small cell tumor. Most patients present with fragility, easy bruising, ecchymoses, and a thin or trans-
itary, causing them to secrete pro-opiomelanocortin signs and symptoms of Cushing’s syndrome before lucent appearance to the skin. Prominent purple to red
(POMC), which is posttranslationally modified into the underlying tumor is diagnosed. This form of striae are seen as a result of the loss of normal connec-
ACTH. ACTH then acts on the adrenal glands to Cushing’s syndrome can be very difficult to differentiate tive tissue function within the skin. The striae are most
increase production of cortisol. Normally, cortisol and from Cushing’s disease in the early stages of each, prominent in areas of obesity and are made more
ACTH both act in a negative feedback loop to inhibit and the clinician needs to be aware of the various noticeable by the central fat redistribution. Facial pleth-
excessive secretion of CRH. pathophysiological mechanisms involved in excessive ora is frequently seen and is likely caused by thinning
Excessive ACTH may be produced in several ways. ACTH production. When faced with a patient with of the skin and an underlying polycythemia. Excessive
Most often, it is produced from a basophilic adenoma excessive ACTH production, the clinician must perform cortisol leads to increased blood glucose levels; this in
of the anterior stalk of the pituitary gland. The term a thorough evaluation, including history, physical turn can lead to poor wound healing and an increase in
232 THE NETTER COLLECTION OF MEDICAL ILLUSTRATIONS