
Page 247 - The Netter Collection of Medical Illustrations - Integumentary System_ Volume 4 ( PDFDrive )
P. 247
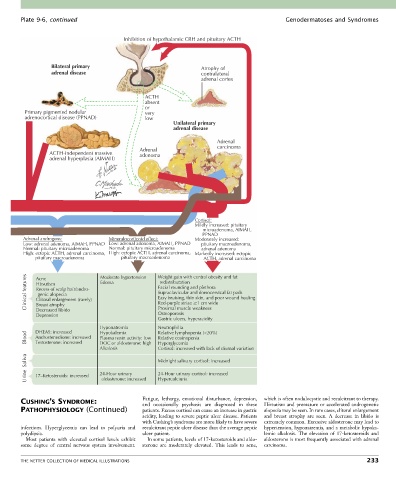
Plate 9-6, continued Genodermatoses and Syndromes
Inhibition of hypothalamic CRH and pituitary ACTH
Bilateral primary Atrophy of
adrenal disease contralateral
adrenal cortex
ACTH
absent
or
Primary pigmented nodular very
adrenocortical disease (PPNAD) low
Unilateral primary
adrenal disease
Adrenal
carcinoma
Adrenal
ACTH-independent massive adenoma
adrenal hyperplasia (AIMAH)
Cortisol:
Mildly increased: pituitary
microadenoma, AIMAH,
PPNAD
Adrenal androgens: Mineralocorticoid effect: Moderately increased:
Low: adrenal adenoma, AIMAH, PPNAD Low: adrenal adenoma, AIMAH, PPNAD pituitary macroadenoma,
Normal: pituitary microadenoma Normal: pituitary microadenoma adrenal adenoma
High: ectopic ACTH, adrenal carcinoma, High: ectopic ACTH, adrenal carcinoma, Markedly increased: ectopic
pituitary macroadenoma pituitary macroadenoma ACTH, adrenal carcinoma
Clinical features Acne Moderate hypertension Weight gain with central obesity and fat
redistributation
Edema
Hirsutism
Facial rounding and plethora
Recess of scalp hair/andro-
Supraclavicular and dorsocervical fat pads
genic alopecia
Easy bruising, thin skin, and poor wound healing
Clitoral enlargement (rarely)
Red-purple striae 1 cm wide
Breast atrophy
Decreased libido
Osteoporosis
Depression Proximal muscle weakness
Gastric ulcers, hyperacidity
Hyponatremia Neutrophilia
DHEAS: increased
Hypokalemia
Relative lymphopenia (<20%)
Blood Androstenedione: increased Plasma renin activity: low Relative eosinopenia
Testosterone: increased
Hyperglycemia
DOC or aldosterone: high
Alkalosis Cortisol: increased with lack of diurnal variation
Saliva Midnight salivary cortisol: increased
Urine 17–Ketosteroids: increased 24-Hour urinary 24-Hour urinary cortisol: increased
Hypercalciuria
aldosterone: increased
CUSHING’S SYNDROME: Fatigue, lethargy, emotional disturbance, depression, which is often nodulocystic and recalcitrant to therapy.
Hirsutism and premature or accelerated androgenetic
and occasionally psychosis are diagnosed in these
PATHOPHYSIOLOGY (Continued) patients. Excess cortisol can cause an increase in gastric alopecia may be seen. In rare cases, clitoral enlargement
acidity, leading to severe peptic ulcer disease. Patients and breast atrophy are seen. A decrease in libido is
with Cushing’s syndrome are more likely to have severe extremely common. Excessive aldosterone may lead to
infections. Hyperglycemia can lead to polyuria and recalcitrant peptic ulcer disease than the average peptic hypertension, hyponatremia, and a metabolic hypoka-
polydipsia. ulcer patient. lemic alkalosis. The elevation of 17-ketosteroids and
Most patients with elevated cortisol levels exhibit In some patients, levels of 17-ketosteroids and aldo- aldosterone is most frequently associated with adrenal
some degree of central nervous system involvement. sterone are moderately elevated. This leads to acne, carcinoma.
THE NETTER COLLECTION OF MEDICAL ILLUSTRATIONS 233