
Page 99 - The Netter Collection of Medical Illustrations - Integumentary System_ Volume 4 ( PDFDrive )
P. 99
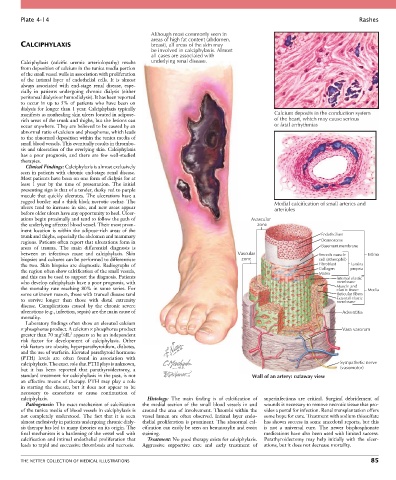
Plate 4-14 Rashes
Although most commonly seen in
areas of high fat content (abdomen,
CALCIPHYLAXIS breast), all areas of the skin may
be involved in calciphylaxis. Almost
all cases are associated with
Calciphylaxis (calcific uremic arteriolopathy) results underlying renal disease.
from deposition of calcium in the tunica media portion
of the small vessel walls in association with proliferation
of the intimal layer of endothelial cells. It is almost
always associated with end-stage renal disease, espe-
cially in patients undergoing chronic dialysis (either
peritoneal dialysis or hemodialysis). It has been reported
to occur in up to 5% of patients who have been on
dialysis for longer than 1 year. Calciphylaxis typically
manifests as nonhealing skin ulcers located in adipose- Calcium deposits in the conduction system
rich areas of the trunk and thighs, but the lesions can of the heart, which may cause serious
occur anywhere. They are believed to be caused by an or fatal arrhythmias
abnormal ratio of calcium and phosphorus, which leads
to the abnormal deposition within the tunica media of
small blood vessels. This eventually results in thrombo-
sis and ulceration of the overlying skin. Calciphylaxis
has a poor prognosis, and there are few well-studied
therapies.
Clinical Findings: Calciphylaxis is almost exclusively
seen in patients with chronic end-stage renal disease.
Most patients have been on one form of dialysis for at
least 1 year by the time of presentation. The initial
presenting sign is that of a tender, dusky red to purple
macule that quickly ulcerates. The ulcerations have a
ragged border and a thick black necrotic eschar. The Medial calcification of small arteries and
ulcers tend to increase in size, and new areas appear arterioles
before older ulcers have any opportunity to heal. Ulcer-
ations begin proximally and tend to follow the path of Avascular
the underlying affected blood vessel. Their most prom- zone
inent location is within the adipose-rich areas of the
trunk and thighs, especially the abdomen and mammary Endothelium
regions. Patients often report that ulcerations form in Desmosome
areas of trauma. The main differential diagnosis is Basement membrane
between an infectious cause and calciphylaxis. Skin Vascular Smooth muscle Intima
biopsies and cultures can be performed to differentiate zone cell (atherophil)
the two. Skin biopsies are diagnostic. Radiographs of Fibroblast Lamina
the region often show calcification of the small vessels, Collagen propria
Matrix
and this can be used to support the diagnosis. Patients Internal elastic
who develop calciphylaxis have a poor prognosis, with membrane
the mortality rate reaching 80% in some series. For Muscle and Media
elastic tissue
some unknown reason, those with truncal disease tend Reticular fibers
to survive longer than those with distal extremity External elastic
membrane
disease. Complications caused by the chronic severe
ulcerations (e.g., infection, sepsis) are the main cause of Adventitia
mortality.
Laboratory findings often show an elevated calcium
× phosphorus product. A calcium × phosphorus product Vasa vasorum
2
2
greater than 70 mg /dL appears to be an independent
risk factor for development of calciphylaxis. Other
risk factors are obesity, hyperparathyroidism, diabetes,
and the use of warfarin. Elevated parathyroid hormone
(PTH) levels are often found in association with
calciphylaxis. The exact role that PTH plays is unknown, Sympathetic nerve
but it has been reported that parathyroidectomy, a (vasomotor)
standard treatment for calciphylaxis in the past, is not Wall of an artery: cutaway view
an effective means of therapy. PTH may play a role
in starting the disease, but it does not appear to be
necessary to exacerbate or cause continuation of
calciphylaxis. Histology: The main finding is of calcification of superinfections are critical. Surgical debridement of
Pathogenesis: The exact mechanism of calcification the medial section of the small blood vessels in and wounds is necessary to remove necrotic tissue that pro-
of the tunica media of blood vessels in calciphylaxis is around the area of involvement. Thrombi within the vides a portal for infection. Renal transplantation offers
not completely understood. The fact that it is seen vessel lumen are often observed. Intimal layer endo- some hope for cure. Treatment with sodium thiosulfate
almost exclusively in patients undergoing chronic dialy- thelial proliferation is prominent. The abnormal cal- has shown success in some anecdotal reports, but this
sis therapy has led to many theories on its origin. The cification can easily be seen on hematoxylin and eosin is not a universal cure. The newer bisphosphonate
final mechanism is a hardening of the vessel wall with staining. medications have also been used with limited success.
calcification and intimal endothelial proliferation that Treatment: No good therapy exists for calciphylaxis. Parathyroidectomy may help initially with the ulcer-
leads to rapid and successive thrombosis and necrosis. Aggressive supportive care and early treatment of ations, but it does not decrease mortality.
THE NETTER COLLECTION OF MEDICAL ILLUSTRATIONS 85