
Page 294 - ACCCN's Critical Care Nursing
P. 294
Cardiac Rhythm Assessment and Management 271
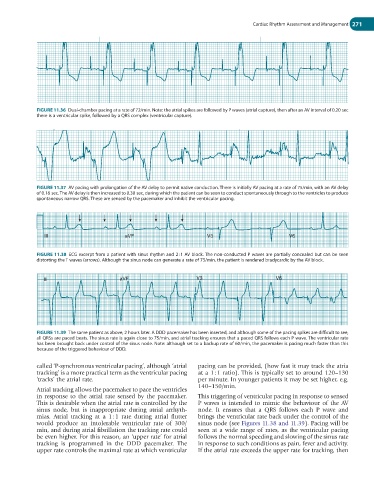
FIGURE 11.36 Dual-chamber pacing at a rate of 72/min. Note: the atrial spikes are followed by P waves (atrial capture), then after an AV interval of 0.20 sec
there is a ventricular spike, followed by a QRS complex (ventricular capture).
FIGURE 11.37 AV pacing with prolongation of the AV delay to permit native conduction. There is initially AV pacing at a rate of 75/min, with an AV delay
of 0.16 sec. The AV delay is then increased to 0.30 sec, during which the patient can be seen to conduct spontaneously through to the ventricles to produce
spontaneous narrow QRS. These are sensed by the pacemaker and inhibit the ventricular pacing.
III aVF V3 V6
FIGURE 11.38 ECG excerpt from a patient with sinus rhythm and 2 : 1 AV block. The non-conducted P waves are partially concealed but can be seen
distorting the T waves (arrows). Although the sinus node can generate a rate of 75/min, the patient is rendered bradycardic by the AV block.
III aVF V 3 V 6
FIGURE 11.39 The same patient as above, 2 hours later. A DDD pacemaker has been inserted, and although some of the pacing spikes are difficult to see,
all QRSs are paced beats. The sinus rate is again close to 75/min, and atrial tracking ensures that a paced QRS follows each P wave. The ventricular rate
has been brought back under control of the sinus node. Note: although set to a backup rate of 60/min, the pacemaker is pacing much faster than this
because of the triggered behaviour of DDD.
called ‘P-synchronous ventricular pacing’, although ‘atrial pacing can be provided, (how fast it may track the atria
tracking’ is a more practical term as the ventricular pacing at a 1 : 1 ratio). This is typically set to around 120–130
‘tracks’ the atrial rate. per minute. In younger patients it may be set higher, e.g.
140–150/min.
Atrial tracking allows the pacemaker to pace the ventricles
in response to the atrial rate sensed by the pacemaker. This triggering of ventricular pacing in response to sensed
This is desirable when the atrial rate is controlled by the P waves is intended to mimic the behaviour of the AV
sinus node, but is inappropriate during atrial arrhyth- node. It ensures that a QRS follows each P wave and
mias. Atrial tracking at a 1 : 1 rate during atrial flutter brings the ventricular rate back under the control of the
would produce an intolerable ventricular rate of 300/ sinus node (see Figures 11.38 and 11.39). Pacing will be
min, and during atrial fibrillation the tracking rate could seen at a wide range of rates, as the ventricular pacing
be even higher. For this reason, an ‘upper rate’ for atrial follows the normal speeding and slowing of the sinus rate
tracking is programmed in the DDD pacemaker. The in response to such conditions as pain, fever and activity.
upper rate controls the maximal rate at which ventricular If the atrial rate exceeds the upper rate for tracking, then