
Page 70 - Textbook of Pathology, 6th Edition
P. 70
54
TABLE 3.6: Differences between Dystrophic and Metastatic Calcification.
Feature Dystrophic Calcification Metastatic Calcification
1. Definition Deposits of calcium salts in dead and Deposits of calcium salts in normal tissues
degenerated tissues
2. Calcium metabolism Normal Deranged
3. Serum calcium level Normal Hypercalcaemia
4. Reversibility Generally irreversible Reversible upon correction of metabolic disorder
SECTION I
5. Causes Necrosis (caseous, liquefactive, fat), Hyperparathyroidism (due to adenoma,
infarcts, thrombi, haematomas, dead hyperplasia, CRF), bony destructive lesions
parasites, old scars, atheromas, (e.g. myeloma, metastatic carcinoma),
Mönckeberg’s sclerosis, certain prolonged immobilisation, hypervitaminosis D,
tumours, cysts, calcinosis cutis milk-alkali syndrome, hypercalcaemia of infancy
6. Pathogenesis Increased binding of phosphates with Increased precipitates of calcium phosphate due to
necrotic and degenerative tissue, which hypercalcaemia at certain sites e.g. in lungs, stomach,
in turn binds to calcium forming blood vessels and cornea
calcium phosphate precipitates
hyperplasia ( postfix word -trophy means nourishment; -plasia the concept of evolution ‘survival of the fittest’ holds true
means growth of new cells). for adaptation as ‘survival of the adaptable’.
Various mechanisms which may be involved in adaptive
Changing the pathway of phenotypic differentiation of
cells i.e. metaplasia and dysplasia (prefix word meta- means cellular responses include the following:
transformation; dys- means bad development). Altered cell surface receptor binding.
Alterations in signal for protein synthesis.
In general, the adaptive responses are reversible on withdrawal Synthesis of new proteins by the target cell such as heat-
of stimulus. However, if the irritant stimulus persists for long shock proteins (HSPs).
time, the cell may not be able to survive and may either die Common forms of cellular adaptive responses along with
or progress further e.g. cell death may occur in sustained examples of physiologic and pathologic adaptations are
atrophy; dysplasia may progress into carcinoma in situ. Thus, briefly discussed below (Fig. 3.39).
General Pathology and Basic Techniques
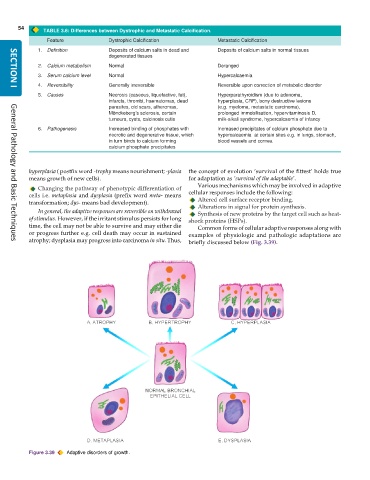
Figure 3.39 Adaptive disorders of growth.