
Page 868 - Textbook of Pathology, 6th Edition
P. 868
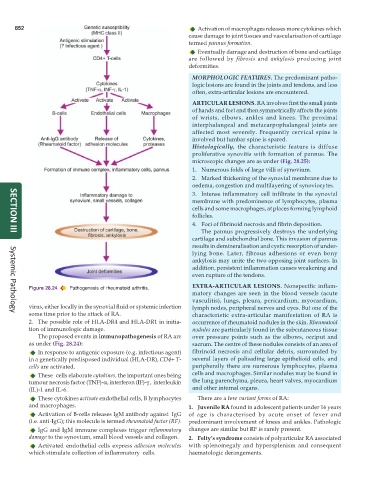
852 Activation of macrophages releases more cytokines which
cause damage to joint tissues and vascularisation of cartilage
termed pannus formation.
Eventually damage and destruction of bone and cartilage
are followed by fibrosis and ankylosis producing joint
deformities.
MORPHOLOGIC FEATURES. The predominant patho-
logic lesions are found in the joints and tendons, and less
often, extra-articular lesions are encountered.
ARTICULAR LESIONS. RA involves first the small joints
of hands and feet and then symmetrically affects the joints
of wrists, elbows, ankles and knees. The proximal
interphalangeal and metacarpophalangeal joints are
affected most severely. Frequently cervical spine is
involved but lumbar spine is spared.
Histologically, the characteristic feature is diffuse
proliferative synovitis with formation of pannus. The
microscopic changes are as under (Fig. 28.25):
1. Numerous folds of large villi of synovium.
2. Marked thickening of the synovial membrane due to
oedema, congestion and multilayering of synoviocytes.
3. Intense inflammatory cell infiltrate in the synovial
membrane with predominence of lymphocytes, plasma
cells and some macrophages, at places forming lymphoid
follicles.
4. Foci of fibrinoid necrosis and fibrin deposition.
The pannus progressively destroys the underlying
SECTION III
cartilage and subchondral bone. This invasion of pannus
results in demineralisation and cystic resorption of under-
lying bone. Later, fibrous adhesions or even bony
ankylosis may unite the two opposing joint surfaces. In
addition, persistent inflammation causes weakening and
even rupture of the tendons.
EXTRA-ARTICULAR LESIONS. Nonspecific inflam-
Figure 28.24 Pathogenesis of rheumatoid arthritis.
matory changes are seen in the blood vessels (acute
vasculitis), lungs, pleura, pericardium, myocardium,
virus, either locally in the synovial fluid or systemic infection lymph nodes, peripheral nerves and eyes. But one of the
some time prior to the attack of RA. characteristic extra-articular manifestation of RA is
Systemic Pathology
2. The possible role of HLA-DR4 and HLA-DR1 in initia- occurrence of rheumatoid nodules in the skin. Rheumatoid
tion of immunologic damage. nodules are particularly found in the subcutaneous tissue
The proposed events in immunopathogenesis of RA are over pressure points such as the elbows, occiput and
as under (Fig. 28.24): sacrum. The centre of these nodules consists of an area of
In response to antigenic exposure (e.g. infectious agent) fibrinoid necrosis and cellular debris, surrounded by
in a genetically predisposed individual (HLA-DR), CD4+ T- several layers of palisading large epithelioid cells, and
cells are activated. peripherally there are numerous lymphocytes, plasma
These cells elaborate cytokines, the important ones being cells and macrophages. Similar nodules may be found in
tumour necrosis factor (TNF)-α, interferon (IF)-γ , interleukin the lung parenchyma, pleura, heart valves, myocardium
(IL)-1 and IL-6. and other internal organs.
These cytokines activate endothelial cells, B lymphocytes There are a few variant forms of RA:
and macrophages. 1. Juvenile RA found in adolescent patients under 16 years
Activation of B-cells releases IgM antibody against IgG of age is characterised by acute onset of fever and
(i.e. anti-IgG); this molecule is termed rheumatoid factor (RF). predominant involvement of knees and ankles. Pathologic
IgG and IgM immune complexes trigger inflammatory changes are similar but RF is rarely present.
damage to the synovium, small blood vessels and collagen. 2. Felty’s syndrome consists of polyarticular RA associated
Activated endothelial cells express adhesion molecules with splenomegaly and hypersplenism and consequent
which stimulate collection of inflammatory cells. haematologic derangements.